
Above: Louis Armstrong Basin Street Blues 1928
I have a real problem with the attention ‘assisted dying’ gets in the media, mainly because I think that if we discussed unequal access to privileged services and underprivileged services through marketing segmentation that we’d have a completely different view of society.
If we agreed that, really we must take economics, cultural and political representation into the hard, difficult parts of society we’d think and see ourselves and everyone, differently.
I think that we’d find a counter narrative that changes everything and everyone.
It’s always been here: the wallpaper of who we think we are: like slaves, indentured servants, immigrants and refugees, we’re all, always here, reaching out for a better, unimagined future of success, connection, feeling valid and valued.
When we create a Brexit company as a political party with directors, we’re not getting democracy, we’re getting more gig and gang labour, more blurring of the legal and illegal supply chains. More county lines and only marketing segmentation that uses algorhythmic predestination but doesn’t change anything for anyone.
Underneath the question of assisted dying is an acceptance that we can’t change anything. But we can. Futility underlies suicide but there’s a structured futility that we have to eradicate.
Under the despairing personal stories of Geoff Whaley Paul Blomfield and political campaigns to ‘ease the legislation’, say of Nick Bowles is an end of democratic, end of times mantra that’s speaking people, speaking through people, writing them off, but actually, long before they despair and commit suicide.
We need to understand where these questions are really coming from. Taking democracy away from the difficult parts of society, avoiding the difficult questions and replacing them with american evangelical organisations, consultants who toddle off to America, Australia or New Zealand to report back on solutions that change nothing are not what is needed.
We need democracy, accountability and enfranchisement.
When Paul Blomfield’s dad committed suicide because he thought he had no choice, his death, in a way, is a terrible wrong, to me, a real sign that we need to rebuild capacity and help our society move beyond its obsession with a labelling, fixing, de capacitating bureaucracy that just gets bigger and bigger.
The post world war two economy valued speed, size and massification as indicators of growth when it’s the scale and overall workforce health in the project construction of health, education, finance, manufacture, construction and infrastructure that needs humanising.
Projects always could have been smaller, more inclusive, more accountable.
Instead we have used quality data, information and knowledge to create a marketing apartheid, a mosaic of fractured and fragmenting characteristics that structure narcissism as a human given and in that confusion make us imagine we are gods when in data terms, increasingly we’re being locked down and determined, whoever we are, whatever our status.
That’s the mentality we call ‘mental illness’ where more people may experience existential despair wherever they are in the social descriptors because really they’re in a neglected space, nothing is growing there, nothing of meaning, development, security and hope grows there. What we’d have called dead boring when we were younger becomes a distorted space where all hell can be let loose on an individual: gambling, crime, drugs, addiction. It happens because we’ve disenfranchised those places.
Increasingly, knowing is in the hands of technologies who determine our jobs. We give our machines grace when they need to give us space.
The direction of our lives, the flow, the detail, the ownership of anything is contested, questioned, interrogated until it’s worthless and people go thrill, attention, and experience seeking, when they know that the real work is there, under their noses, the social questions that need their attention are forever ignored, frustrated in ever more sophisticated re iterations of ‘the work’ that needs to be done.
Increasingly, in this locally forgotten space, filled now by religious groups, charities there’s an end of times narrative to their contribution and they turn an already moted eye away from the hard job of really creating new sustainable jobs and opportunities that might lessen dependancy.
When they see the blurring of lines between legal and illegal supply chains and strange kinds of control over mass markets in race, sex, age and class in the local environment they don’t see the problems in terms of a local economic, social and cultural history of exclusion. And they need to recognise that there needs to be economic, social, political and cultural accountability and representation in these spaces.
Think about war veterans, refugees and immigrants after the second world war numb, battered from their experiences and suddenly there’s light: the Festival Of Britain: making, beauty, aesthetics, renewal.
What people have lost and need to regain is a sense that everyone matters, projects that are small and connecting have always been on the agenda, throughout the periods before wars, during and after them: look at the social conditions in London during the second world war that artist Abram Games attempted to document but that Winston Churchill suppressed. Abram, whose parents were Latvian and Polish Russian refugees to London in 1904, produced war posters that didn’t just talk about the value of fighting for war, they introduced the complexity of the poverty at home and how there was a need for reconstruction.
Churchill banned this poster which drew a complex image of social questions, poverty existing simultaneously with the threats of war:
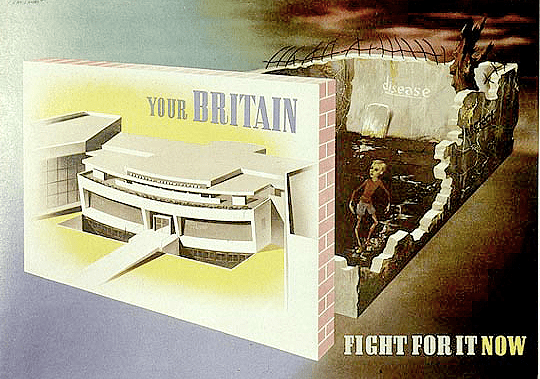
Above: Abram Games image of the social reconstruction at home needed simultaneously with the need to fight in the war which Churchill found so overwhelming: he ordered that it be removed.
When you think about the complexity of Churchill’s mentality and his ambivalence: when the debating chamber was bombed, though, the architect, the artist, the creative in him argued:
‘We shape our buildings, and afterwards our buildings shape us.’
He was against ‘giving each member a desk to sit at and a lid to bang’ because, he explained, the House would be mostly empty most of the time, whereas, at critical votes and moments, it would fill beyond capacity, with members spilling out into the aisles: in his view,a suitable ‘sense of crowd and urgency’ (Churchill, 1943). The Psychologist, Feb 2009
When we talk about mental health, depression, ambivalence, we’re also talking about sensitivities where someone like Churchill would be caught between a loving, creative, awareness of human potential and a the wilful shutting out of potential, possibilities, the ‘other’ -other ways of thinking, feeling, behaving, doing and making things because he had to be a leader, had to represent a view of the world that had the empathy knocked out of it.
When you think how in peace, just as Margaret Thatcher and now, Teresa May experienced; Churchill was also jettisoned by the Conservative party. Since the second world war all social change has coalesced around the unwillingess of psychologically feudal systems of privilege to move beyond war and demand planning into local representational mosaics that include a richer history, capacity and potential. People centred, smaller, more human.
When people sketch, draw, music, play, dance, congregate in cities it feels as if we are in peace at a time of war, rehearsing better ways of working and living, smaller, less bureaucratic: when people feel pain, distress, mental illness it’s because they’ve been de capacitated, disenfranchised.
It’s really important to respect privilege but also to understand its limitations. We need to be the archaeologists of local truth, connection and also to be the diviners of where the flows are, the new, the histories and where they may blend to create more human ways of working and living.
When you think about post war design companies like Schreiber who grew into a burgeoning culture in the seventies where companies began to plan for the next hundred years, think about who, why, where that kind of planning would be a threat.
All I can think of is that is when companies began to plan only a few years ahead and we now see that as a norm, we’ve also forgotten what it might feel like to idly dream, to see into the blue, over the horizon.
I think that the fearfulness that people seem to take home from work is eroding some essential part of our humanity, our human aspirations. I think the systems around us curtail and time limit us.
We’re in a monitored, gelatinous bureaucracy around economic movement and activity we live inside a mosaic of social segmentation that needs to be challenged and enriched with alternatives inputs that create human and humane jobs and life cycles.
In this view some people have overdetermined access to hope and optimism because of it, others have overdetermined connections to despair and pessimism because of it.
Neither are what we need.

The BMJ has provided a platform for debate on assisted dying since 2002
2018
- News: Assisted dying: Guernsey rejects proposal to move towards legalisation
- BMJ Opinion: End of life care—the assisted dying debate continues
- Editor’s choice: Assisted dying: it’s time to poll UK doctors
- Personal view: Most UK doctors support assisted dying, a new poll shows: the BMA’s opposition does not represent members
- Commentary: Palliative care and assisted dying are not mutually exclusive
- Feature: Assisted dying in US and Canada: controversy subsides after legalisation
- Essay: How it feels to help a terminally ill patient to die a dignified death
- Patient Commentary: “I don’t want to go to Switzerland, and I don’t want to attempt suicide”
- Head to head: Should doctor assisted dying be legal?
- BMJ Opinion: Assisted dying—how safe is safe enough?
2017
- Personal view: Why I’ve changed my views on assisted dying
- Letter: Assisted death in “healthy” old age needs consideration
- Analysis: Assisted dying for healthy older people: a step too far?
2016
- Analysis: Embracing inherent uncertainty in advanced illness
- Editorial: End of life care still not living up to public and doctors’ expectations
- Personal view: My mum’s decision changed my view of assisted dying
2015
- Letter: Matters arising from The BMJ’s stance on assisted dying
- David Oliver: What to do about end of life scare stories
- Letter: The BMJ’s views on assisted dying: non-representative of its audience
- Letter: The Assisted Dying Bill is not a UK bill
- Editor’s Choice: Assisted dying—time for a full and fair debate
- Head to head: Would judicial consent for assisted dying protect vulnerable people?
- Personal view: Assisted dying: legal ambiguity lets down families as well as patients
- Personal view: Mental capacity as a safeguard in assisted dying: clarity is needed
- Feature: Assisted dying: law and practice around the world
- Feature: A doctor who chose an assisted death
- Feature: In support of assisted dying
2014
- Letter: Data to support assisted dying
- Letter: No man is an island
- Letter: Why The BMJ should not declare a stance on assisted dying
- Letter: Why public opinion should not enter the debate about assisted dying
- Letter: Attending to the vulnerabilities of people who are dying
- Letter: Widening the net of assisted suicide to vulnerable people
- Letter: Why the Assisted Dying Bill is not needed in England and Wales
- Letter: Assisting suicide goes against why most of us became doctors
- Letter: Some data on assisted dying from Oregon are worrying
- Personal view: An assisted dying law might save me from a lingering and unpleasant death
- Letter: “Misleading falsehoods” regarding assisted dying?
- Margaret McCartney: The BMJ is wrong: doctor assisted dying would overmedicalise death
- Editor’s Choice: Choice in matters of life and death
- Observations: We must not deprive dying people of the most important protection
- Editorials: Why the Assisted Dying Bill should become law in England and Wales
- Letter: The limits of palliative care
- Letter: RCGP consultation on assisted dying was comprehensive and conclusively in favour of no change to the law
- Editorials: Why is talking about dying such a challenge?
- Observations: Assisted dying is not the same as euthanasia
- Letter: All RCGP members should be balloted on assisted dying
- Feature: The end of life
2013
- Letter: The Swiss experience of assisted suicide is positive
- Letter: Giving dying people what they want
- Letter: What do families and professional organisations really think about assisted dying?
- Letter: The law should be changed to allow assisted dying
- Personal view: Legalising assisted dying puts vulnerable patients at risk and doctors must speak up
- Feature: Assisted dying: what happens after Vermont?
2012
- Letter: Not all “good” doctors do it anyway
- Letter: The “least worst” course of action?
- Personal view: Assisted dying: “all good doctors do it anyway”
- Personal view: Terminally ill people shouldn’t have to travel abroad for assisted dying
- Letter: A carefully crafted law should protect and reassure vulnerable people
- Letter: Abortion reform’s lessons for assisted dying
- Letter: Safe laws on assisted dying are working worldwide
- Letter: My journey from anti to pro assisted dying
- Letter: Why neutrality on assisted dying is not an option for doctors’ professional organisations
- Letter: Editorial note on results of assisted dying poll
- Observations: Our professional bodies should stop opposing assisted dying
- Personal view: My mum wanted assisted dying but we watched her die slowly and in pain
- Editorial: Assisted dying
- Letter: Doctors need to perfect the art of allowing patients to die with dignity
- Letter: Legislation and debate are needed
- Letter: Malign individuals would probably be identified with legislation
- Letter: Consider suffering associated with lack of control over dying
- Letter: Where’s the evidence for malign relatives, professionals, or carers?
- Observation: What’s wrong with assisted dying
- Letter: Does the BMJ have a particular ideology to pursue in assisted dying?
2011
- Letter: So, farewell then, doctrine of double effect
- Letter: My experience with euthanasia
- Letter: Missed opportunity to advance debate on assisted dying
- Letter: Call for an evidence based debate on assisted dying
- Observation: Assisted dying: are doctors in denial?
- Personal view: Assisted dying: we are not alone
- Letter: Assisted dying versus assisted living
- Letter: Tallis’s slippery slope
- Letter: European-wide debate needed
- Letter: Anti-euthanasia cards
- Letter: Better framework needed
- Letter: Try another approach, BMJ
- Letter: What of virtue and integrity?
- Letter: Put everything out in the open
- Letter: Let’s get the words right too
- Letter: Time to be neutral?
2010
- Des Spence: A death of reason
- Des Spence: Talking about a revolution
- Personal view: Assisted suicide: a substitute for a caring doctor?
- Letter: A step backwards?
- Letter: Do it properly or not at all
- Editorial: Doctors and assisted suicide
- Letter: Suicide and euthanasia paradox
- Research: Reporting of euthanasia in medical practice in Flanders, Belgium: cross sectional analysis of reported and unreported cases
- Spotlight: Dying matters: let’s talk about it
- Spotlight: Achieving a good death for all
- Observation: Care Not Killing
- Observation: Half truths and one and a half truths about assisted dying
- Letter: RCA clarifies its position
- Letter: RSM is independent
2009
- Letter: Clinicians need clarification
- Letter: Time for safety and consistency
- Letter: The issue is patient safety
- Research: Euthanasia and other end of life decisions and care provided in final three months of life: nationwide retrospective study in Belgium
- Editorial: End of life decisions and quality of care before death
- Personal view: An extremely interesting time to die
- Editor’s choice: Let’s talk about assisted dying
- Feature: Assisted suicide: the fight goes on
- Editorial: End of life care in the acute hospital setting
- Letter: Doctors, steer clear
- Letter: Observations: Assisted dying: what’s disability got to do with it?
- Letter: A baroness replies
- Letter: Authors respond to editorial
- Letter: Doctors can be trusted
- Letter: Life is a terminal condition
- Letter: Doctors’ attitudes surveyed
- Letter: Doctors, steer entirely clear
- Letter: Counting end of life decisions
- Editorial: Death and dying
- Editorial: New interim guidance on assisted suicide
- Personal view: Letting go
- Research: Concept of unbearable suffering in context of ungranted requests for euthanasia: qualitative interviews with patients and physicians
- Personal view: Euthanasia and free speech in Ireland
2008
- Letter: Please, don’t forget ethical responsibilities
- Letter: Dutch research reflects problems with the Liverpool care pathway
- Analysis: Development of palliative care and legalisation of euthanasia: antagonism or synergy?
- Editorial: Continuous deep sedation in patients nearing death
- Research: Continuous deep sedation for patients nearing death in the Netherlands: descriptive study
- Research: Prevalence of depression and anxiety in patients requesting physicians’ aid in dying: cross sectional survey
- Letter: Euthanasia and depression: no surprise
- Letter: Depression in terminal illness
- Letter: Psychiatric review is mandatory in Australia
- Editorial: Depression and physician assisted dying
- Observations: Paving the way for assisted suicide
- Practice: The last wish of a patient with end stage chronic obstructive pulmonary disease
2006-2007
- Editorial: Physician assisted death in vulnerable populations
- Letter: Are we asking the right questions?
- Editorial: Euthanasia in neonates
- Letter: Double effect is a myth leading a double life
- Analysis: Role of non-governmental organisations in physician assisted suicide
2005
- Letter: RCGP is not neutral: it opposes a change in legislation
- Letter: Response from the Association for Palliative Medicine
- Letter: BMA should take an active role, whatever that may be
- Letter: What autonomy really means
- Letter: Do we make decisions by our feelings or the truth?
- Letter: No, thank you
- Letter: Recruiting more vulnerable doctors may be the answer
- Letter: Use of Baxter products in figure for physician assisted suicide was inappropriate
- Letter: Doctors cannot simultaneously be patient centred and reject assisted suicide
- Letter: Time to legalise assisted dying? : Summary of responses
- Editor’s choice: A time to die
- Education and debate: Time for change
- Education and debate: Legalised euthanasia will violate the rights of vulnerable patients
- Education and debate: Changes in BMA policy on assisted dying
- Education and debate: Moral dimensions
- Education and debate: Dutch experience of monitoring euthanasia
- Education and debate: Legal view of right to life and death could threaten philosophy of palliative care
- Education and debate: Sensitivity and humility are needed when dealing with dying people
- Education and debate: No man (or woman) is an island
- Letter: “Right to die”: Summary of responses
- Editorial: “Right to die”
- Review: Whose Life is it Anyway?
- Education and debate: Timers on ventilators
2004
- Recent developments: Suicide in older people
- The Good Euthanasia Guide 2004: Where, What, and Who in Choices in Dying
- Am I breaking the law again?
- Assisted suicide
2003
- Dead issue
- Oregon update
- Doctors’ opinions on euthanasia, end of life care, and doctor-patient communication: telephone survey in France
- Doctors should not discuss resuscitation with terminally ill patients
- Patient centred death
- Effects of euthanasia on the bereaved family and friends: a cross sectional study
- National survey of medical decisions at end of life made by New Zealand general practitioners
- Patients’ voices are needed in debates on euthanasia
- Law needs to be changed to allow terminally ill people choice of a dignified death
- Do we really know what happens in this country?
- Both how and when determines a good death
- Doctors occupy special position
- Doctors should keep out of it
- “Comfort care” needs robust moral framework
- Distinction needs to be made between choice and obligation
- Assisted suicide and euthanasia in Switzerland
- Death in a consumer society
- Allowing a role for non-physicians
- Lethal injection: a stain on the face of medicine
The counter narrative is?

You must be logged in to post a comment.