
Featured Image: 111 Calls By Top Symptom Group: there’s also GP Level data produced by NHS Digital which looks at scheduled telephone and surgery appointments and things like telephone triage, online consultations, home visits, immunisations, enhanced access appointments. St George’s Medical Practice in WB is sensitive to the way online services can be used and will be developing its online access in a patient focussed way.
Life is precious (see Charlie (11) care of a Mayfly):

And we’re all learning as we go through our lives: the brilliant work of St George’s Patient Forum over the years has helped grow the idea of Integrated Health Care and the plan for Future Health that’s involving more and more of us in the place we want to be part of, develop, share with others (see below):
Held at Rushcliffe Arena the meeting was full of people of all ages who had responded to the NHSNoReply text: ‘St George’s Patient Forum is holding its AGM on the 5th June Chamber B Rushcliffe Arena Rugby Road WB NG2 7HY’.
The Chair of the PPG explained that there’d been so many changes since the last AGM bubbling under the surface of Covid, the long awaited Integrated Health Care Plan for Rushcliffe (see above) that the meeting would take the form of a summary of important info from one of the partners Dr Matt Jelpke and the same from Morgan Sharpe Social Prescribing Team Leader (Bsc Nutrition and Exercise+ 15 years of community health development).
You can probably get Matt’s presentation from Carole Wilson the Practice Manager: it started with the cultural, economic, social environment (we might not realise can be measured). These are Belgian stats- you can find the whole report here
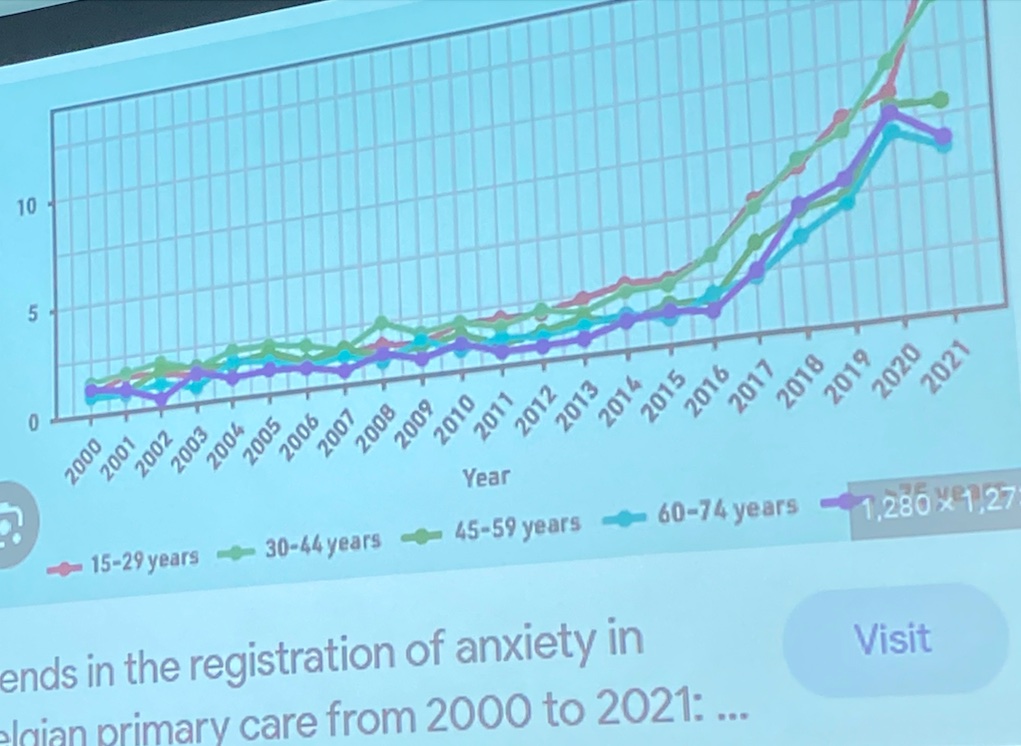
It made me think: so much has altered in the last twenty years: intergenerational relationships, ways of working, living, communicating, spending, leisure. What medicine is, could and should be has also been under intense discussion and scrutiny in that twenty year period.
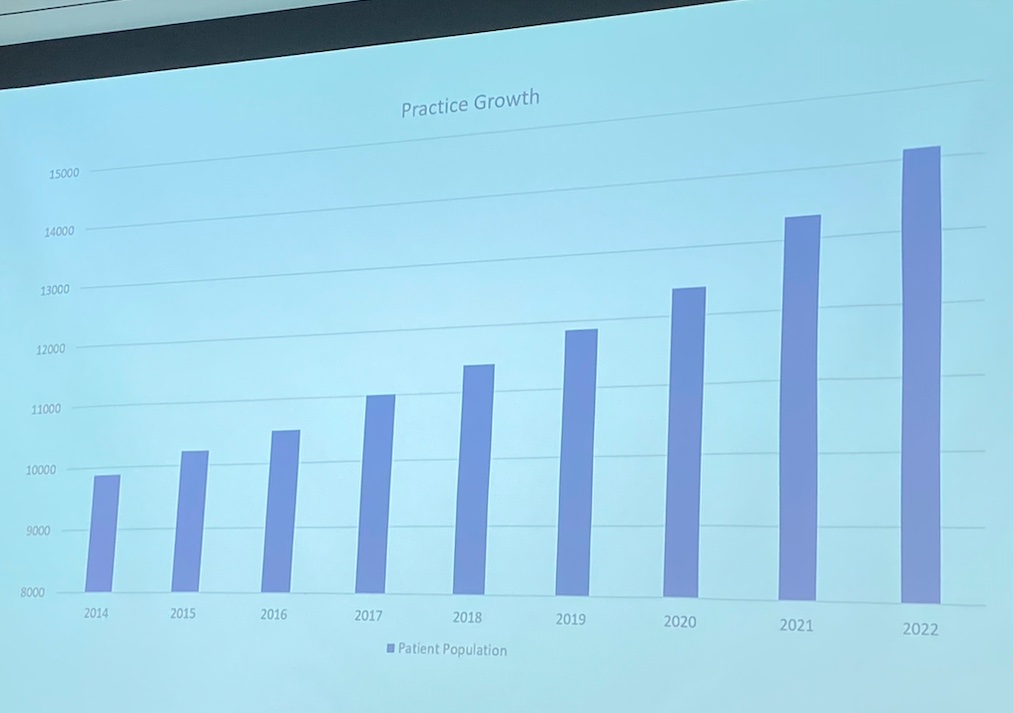
Above: A Bar Chart representing how St George’s Medical Practice has absorbed all the inward migration and housing development in our area in the last nine years. The Practice now has 14,000 patients and is part of a place based seventeen member GP led Community Interest LLP that includes the Musters and Castle Healthcare practices on Wilford Lane.
Although the Registry Office is great: weddings and functions looking out onto the park, when the new health centres were planned I wondered why Musters and St George’s couldn’t have merged with Castle into a central green site like Central Avenue.
It would have been great to have had an architect designed health centre where both practices could create interesting and useful economies of scale: and move away from medicalisation into inclusionary preventative medicine.
The former social services office wasn’t developed to provide a low carbon, multi purpose, multi disciplinary health centre as the catalyst for a new kind of economy starting in West Bridgford.
Our area is affluent (but with the same health, social and economic inequalities as the wider Nottinghamshire area though they’re hidden in the way our community accesses health.
As a Nottingham person I know how in the post second world war era how you’d move from one part of Nottingham to another as you earned more, got married had children): social and economic mobility was comprehensive, creating a rhythm and a culture of progression across society.
In some way though, over the last forty years the value of assets over the people who build and compose that economy has become skewed: in the centre of Nottingham there has been a move away from the traditional housing of students into the global developer business and peripheral student pound driven night time economies, siloed relationships, constant pressure and the impact of that on the health of the students, local householders, employees and employers.
In Rushcliffe we have an economic focus on the power of the older affluent pound and the cost of residential, nursing and home care.
Yet there has always been a history of connection across the city, county, Rushcliffe, district, parish boundaries that we need to reappraise and restore.
Neither of these apparently different economies have grown out of what those individuals or groups aspire to or want. Maybe this is the reason for our anxieties across Rushcliffe/Nottinghamshire borders.
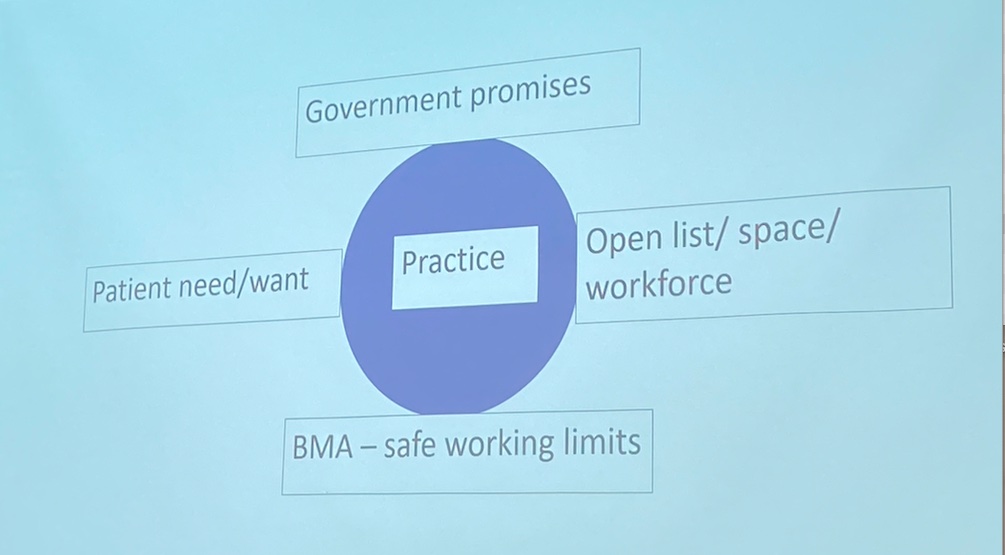
Dr Jelpke’s presentation showed how it feels to be responsible for 14,000 people’s health under these conditions.
What I found so striking is how this really shows the positive and the negative in language that we all experience in our lives on a daily basis: we forget the history of parliamentary representation through a loss of trust in the way government understands its accountabilities, the BMA Safe Working limits aims to reduce the anxieties of medical professionals in meeting the needs of patients: it’s seen as safe for doctors to be in direct consultation with patients for three hours a day and one hour ten in non contact time.
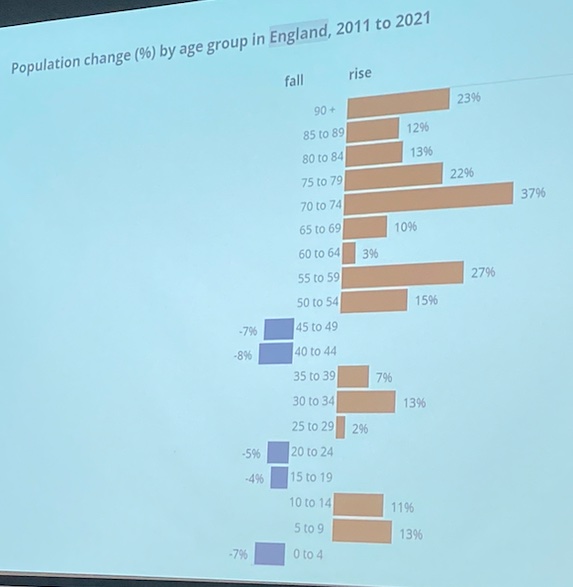
When we consider the impact of the new kinds of economies on health, illness and death in the period 2001-2018 it maybe that we’re becoming aware that in all areas of life: in planning work, building homes, education, skill development, implementation of technologies we need a shared mental model, a sharing, distributive way of teaching, listening and learning from each other so we can make things work better for more people, more of the time.
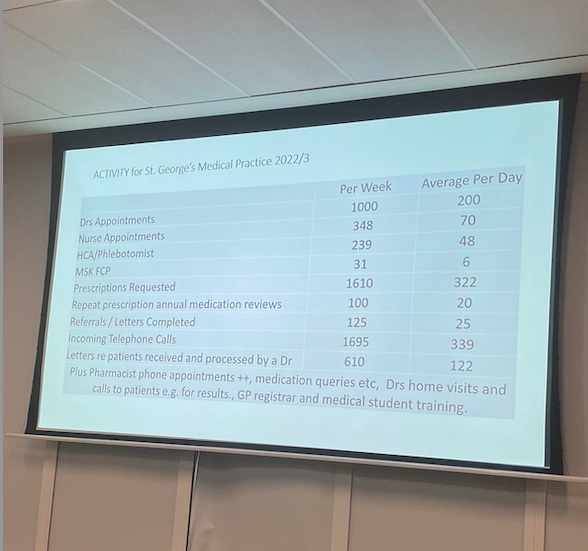
When we look at the practice we visit we can see the pressures: Current BMA standards for a session of GP care is 4 hours 10 minutes. No more than 3 hours of this should be spent in consultation with patients. Within these limits, adequate rest breaks must be taken. St George’s Medical Practice list is 14,000 patients: below is an at a glance list of staff:
You can see from the data for surgery and admin contact averaged each week in the last year: Doctor, Nurse, Health Care/Phlebotomist, Muscoskeletal conditions, Prescriptions (and repeats, reviews), admin, letters, referrals, home visits, calls to patients, GP, registrar and medical student training.
Each one of these services are delivered by the team within the wider team of the wider health service. Doctor Jelpke pointed out that there’s a difference between hospital doctor recruitment and GP recruitment: see below:
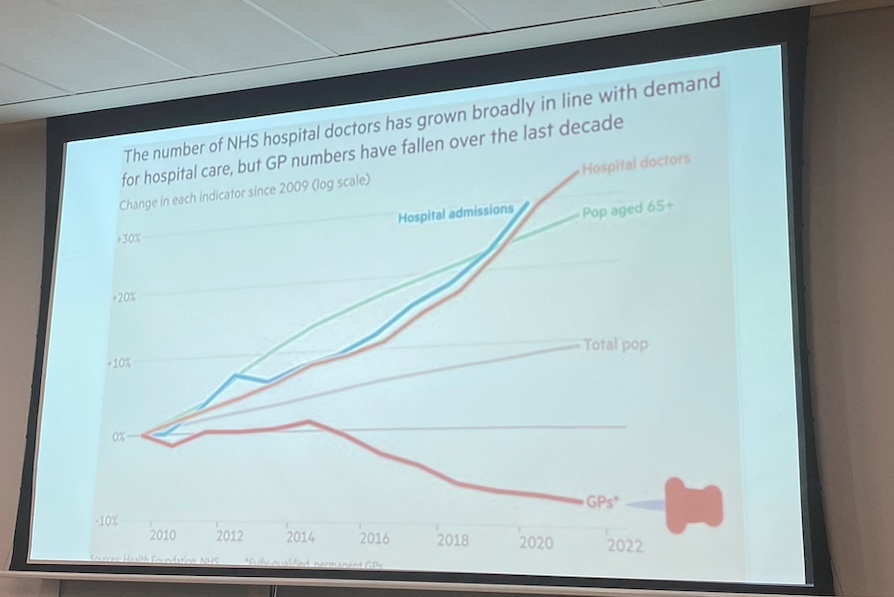
There are many reasons for the recruitment disparities across health services I would imagine: the recruitment of overseas doctors on particular types of contracts, recruited in particular ways and terms: the range of opportunities within hospitals, see below:
Recruitment at the GP practice level I would imagine, is relational, is able to aspire to the common good: there’s a strong conversation going on in GP practice medicine about diverse opportunities and flexibilities, yet it’s confounded by the lack of government appreciation of the investment needed to build workforce capacity to deliver effective preventative health care staff know is needed, doctors know should be there. Dr Jelpke, before introducing Morgan Sharpe, Team Leader for Social Prescribing, talked about the practice’s aspirations to implement person centred technology, talked about aspirations for workforce development but also mentioned how hard it was to recruit receptionists. When you think about St George’s Medical Practice it’s worth thinking of them as a workforce wanting to be better, working in a service for people, with people. The skills, experience and development of this workforce needs to be at the heart of its own understanding of its vision. Social Prescribing is very successful here: I wonder whether career development for reception, admin, secretarial staff into Social Prescribing as well as looking at how the wider hospital careers and GP careers can share, develop, grow higher medical skills giving everyone a workplace reason to use technologies to reduce bureaucracy, differentiation of patients and treatments.
Dr Jelpke introduced Morgan Sharpe (here’s the St George’s Social Prescribing info)
Morgan Sharpe is Rushcliffe Social Prescribing Team Leader looking after North, South and Central Rushcliffe. In the north her team are Gwynneth Owen, Caitlin Jones, Laura Steed, in central, Kasia Frankowska, Sophie Taylor, Fiona Turner, in Central Rushcliffe Nick Marlow, Leanne Hennessey, Jenny Smeeton and the Social Prescribing Care Coordinator is Jackie Kendrick. Morgan has a BSc in Nutrition and Exercise Science and has fifteen years experience in community development project working. The teams have been carefully and sensitively chosen from practitioners in business, mental health, peer to peer work, social work case work, psychologies: all professions undergoing and contributing to career and social change so they’re full of beans and enthusiasm as well as high levels of professional experience and competence. What do they do? Work with people on a one to one basis (like an embodiment of community in a person: your good friend why not, why can’t you? Have you heard of this, With your experience…) they signpost you to people who can help, assist you improve your health, help you regain your enthusiasm and energy for life.
Social Prescribing can help you enjoy food, relaxation, companionship, sleep and get in to a better situation where you can really enjoy and appreciate yourself and others.
Megan and the Rushcliffe team have encyclopaedic knowledge of our area, people, contacts, networks and are at our service. I was incredibly impressed and pleased to have attended the St George’s AGM and want to do everything I can to help them, support them in developing the practice, the workforce and the health of everyone.

You must be logged in to post a comment.